
Date First Published: July 21, 2014
Date Last Revised: January 12, 2024
FUNCTIONS OF THE ORDER ENTRY – RESULT REPORTING (ORDER MANAGEMENT) SYSTEM
The Order Entry System although often termed as Clinical Provider Order Entry (Computerized Physician Order Entry, CPOE), is part of a system that serves four (4) main functions.
- Order entry (planning of a task)
- Task listing (Creation of Worklists)
- Task performance
- Result reporting
- Assigning charges to tasks performed
As such the more correct name for it would be the ‘task management system’, order entry being only one of its components.
Care providers perform their work by completing various tasks or processes. Actually, orders refer to requests, instructions, or intentions to perform tasks. Through them, a care provider records his/her own plans and makes them known to other care providers, inviting them to be involved in the care of the patient. Once made, orders become tasks to be performed. The tasks are listed as worklists and based on which they are addressed one by one by the person responsible to perform them. A completed task would have a result which can be in the form of success (completion) or failure of performance or the data generated. Each task can be given a charge which can be billed once the task is performed.
Types of Orders
In clinical practice orders are made for two main category of services
- to perform a task
- to supply items
Tasks can be clinical tasks such as an interaction with a patient (a consultation), monitoring, performing a procedure or a clinical test, administering a drug. Many tasks are tests or measurements such as laboratory tests, imaging procedures, endoscopy, optometry, audiometry, physiological function tests (e.g. spirometry, cardiac exercise tests, urinary flow tests). Surgery and other procedure related to it are common in patient care.
The items requested through orders include:
- drugs
- consumables
- blood products
- food and beverages
Links to Other Applications and Systems
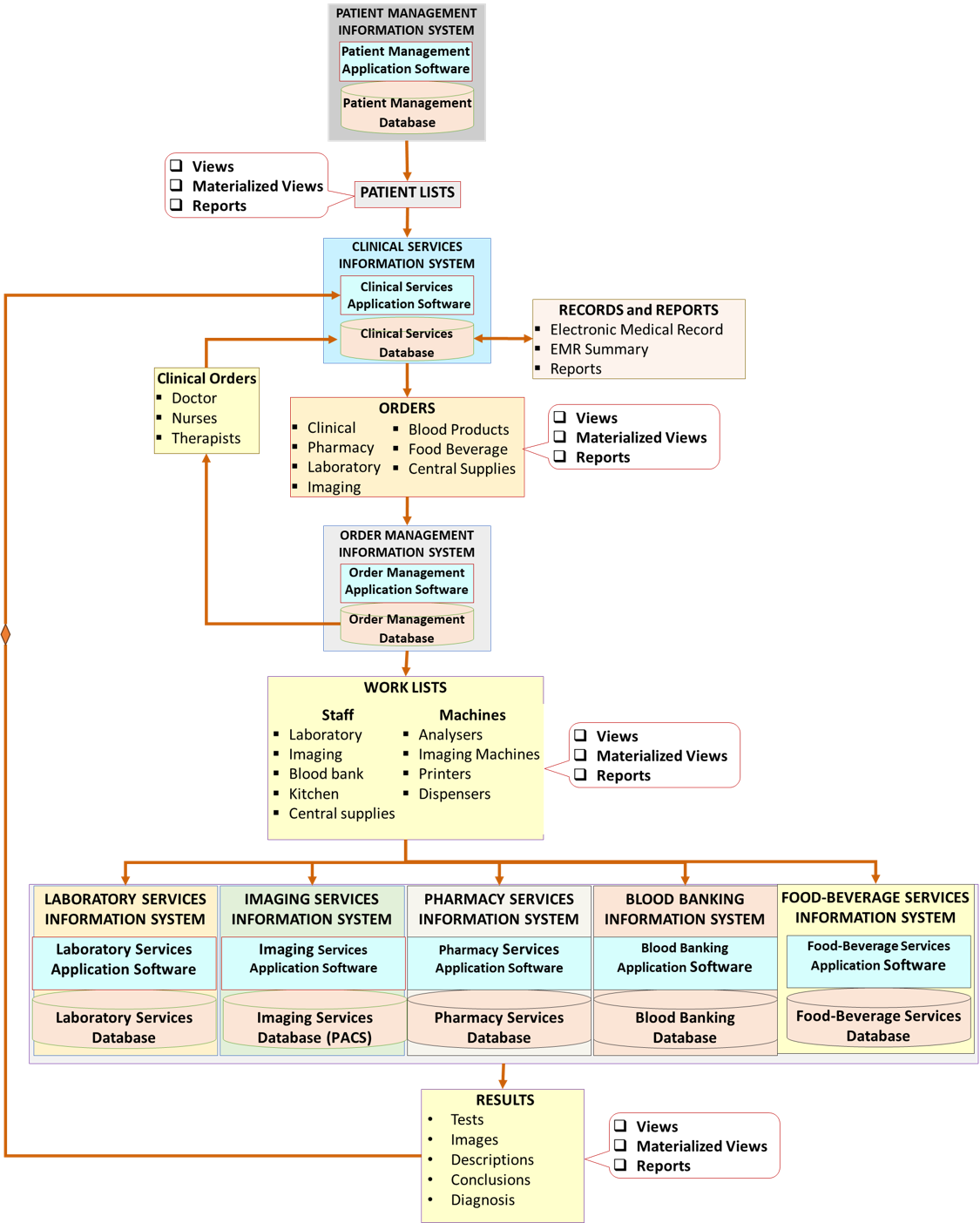
The Order Entry System integrates Clinical Information System (CIS) with Clinical Support Systems and with the Charging and Billing System. The order entry functionality enables clinicians to place an order by selecting it from a list on a menu within the Clinical Information System, instead of from each individual Clinical Support System (Laboratory / Radiology / Pharmacy etc.). The menu groups orders for different tasks. The variations in how orders are processed are discussed under the Clinical Information System (CIS) and various Clinical Support Service Systems (LIS, RIS, Blood Banking, and PhIS).
When necessary and especially for procedures, the order entry application is linked to the Appointment and Scheduling application to ensure that resources are available to carry out the order especially for certain tests like surgical operations, biopsy (FNAC), X-ray examinations and endoscopy.
When an order message is to be transferred to a third-party software (e.g. that of machines or printers), the order management system is interfaced and integrated with the latter, such that the order will create task lists containing all relevant accompanying information. Examples include the creation of work lists on X-ray, Ultrasound, Echocardiography and ESWL machines.
The Order Entry (OR) Application, Server and Database
The order entry functionality can be made part of the various patient care applications such that each application uses its own order mechanism. However, the workflow and data elements used are quite similar making it possible for all the applications to use a common order management application and database. To place an order, clinical providers access the Order Entry application from within the Clinical Information System (CIS) via a menu item labelled as Order entry and the order functionality is made available to them. The care provider will then be a user of the Order Management application in a seamless manner.
The applications receiving the applications need to respond to the Order Management application by:
- acknowledging receipt of the order
- creating task lists based on the orders
- Report that the task has been performed successfully or otherwise.
These three steps will enable the Order Management application to confirm the status of the order (ordered, received/transferred, acted on, completed). The clinical provider can view the status by accessing the Order Management application again. However, the fact that an order has been made, acted on and completed should also be recorded in the CIS and later in the EMR. This is done by the replicating the data in the Clinical Information Database (Clinical Data Repository) which is an operational Database of the CIS.
Once each of the applications has performed the tasks that were ordered, the result obtained is sent to and captured in its own database. It is not necessary to transfer the result to the Order Management system. Instead, the result should be transferred to and replicated in the Clinical Information Database (Clinical Data Repository). This allows the data to be viewed by care providers through their own application i.e. the CIS.
The Order Management application is therefore a separate application with its own database (DBMS, data server and data storage device).
Exception for the Ordering of Drugs
The ordering of drugs is distinctly different from ordering other items. The difference is that it is a prescription rather that just an order. The policies and procedures governing it include:
- Checking validity (appropriateness,availability etc.) at the very beginning,
- Linking to an entire drug database instead of a standard list of orders
- More intense interaction between the order system and the CIS e.g., the drug dispensing and administration process.
For this reason, placing drug orders requires its own specially designed ordering system commonly termed as e-Prescribing. This is discussed in the article the Pharmacy Information System.
CHARACTERISTICS OF ORDER MANAGEMENT SYSTEM
The Order Management system contributes to efficient, effective, appropriate and safe patient care by providing the means to:
- Facilitate communications between various care providers, enabling a care provider to request or instruct another care provider to perform a task or declare his/her intentions regarding what he/she plans to do,
- Promote uniformity of work processes and naming conventions through selection of orders from standard lists
- Enable patient care plans to be converted into executable processes via combinations of orders and tasks (care sets and order sets)
- Initiate and automate processes performed by computers, computer accessories and machines
- Enable the creation of work lists that delineate and assign responsibilities to various care providers involved in direct and supportive care
- Provide instructions and guidance on prerequisites and expected complications of tasks such as tests and procedures
- Ensure that orders are carried out and results obtained by mandating the recording of the outcome (status) of orders
- Link orders and task performance with charges
Orders as Means of Communication
Patient care demands complex relationships between the direct care providers with each other and with the clinical support service providers plus also the clinical administration staff. The Order Management facilitates communications through data sharing and the dissemination of consults, requests, orders and instructions. In a computerized system, these communications initiate or automate work processes or tasks depending on the appropriate situation. The expected outcome of orders are:
- the performance a task that was ordered
- change of status of the order from pending to performed, in progress or completed
- results (Clinical findings, Results of Laboratory test, Diagnostic Imaging, Endoscopy, Special Physiological tests)
- provision of supplies (Medication, Diet, Blood for transfusion, Instruments/Equipment)
A care provider may declare his/her plans by placing the order for the task he/she intends to perform him/herself.
Ordering, performing tasks and reporting of results are essential activities of the patient care service and this sequence of steps need to be followed stringently:
- Select and place orders from list of orders (planned or ad hoc)
- Create task lists or work-lists
- Perform tasks and communicate task completion status
- Document outcome and results
Order-Task Result Sequence

Use of Standard Lists of Orders
Orders need to be specific and unambiguous. The OERR/CPOE system is equipped with tools that enables users to develop Reference Tables containing the hospital’s own Standard List of Orders. The use of these by clinicians confers the benefits of:
- Standardization of nomenclature of orders
- Standardization of tasks or set of tasks that an order is linked to
- Clarity of communication between care providers through the use of standard nomenclature
- Routing of the order to the right place, machine or person
- Attachment of further information and values to the order (e.g. order details, instructions and charges)
- Decision support via prepared reference information or instructions (normal range, warnings if levels are beyond acceptable limits)
- Analysis of data regarding orders (e.g. for quality control and audit)
Orders need to be derived from universally acceptable standard coded lists or at least mapped to them in order to:
- achieve interoperability between sister organizations,
- enable sharing of data with other databases, and
- ensure that data submitted to central bodies especially the government comply with data standards,
When displayed, the standard list (catalogue of orders) can be further broken up into smaller groups or sub-categories according to order types. Hence, customized views can be created for user groups and even individual care providers (e.g. favourites list).
Orders can be made ad hoc or planned as part of a Care Plan.
Tasks are usually performed according to orders. At certain occasions (e.g. in an emergency) tasks may be performed ad hoc without an order. This practice should be discouraged.
To promote smooth operations, the OERRS should facilitate the following functions:
- Performance of tasks based on orders
- Authorization and assignment of responsibility,
- Record of the time interval between various steps of the task beginning from the planning of a task until the actual performance
- Indicate the status of completion of the steps and the whole task
It is important to note that orders can be grouped and given a group name (compound orders, order sets). A compound order can initiate or mandate more than one task. For example an order to collect a laboratory specimen would automatically initiate an additional task i.e. for the printer to print a label.
Order Types
The order entry functionality should be able to process order types in the following ways:
- single order
- initiate or mandate more than one task with an order (compound order)
- order a group of tasks/tests to be performed together at one go with multiple results e.g. LFT, Renal profile (order panel for an analyser)
- several orders ordered together, not necessarily to be performed at one go or by the same person or machine (order sets)
- enable an order to placed but activated only at the next visit /later date (future orders)
- enable an order to be repeated at desired frequency and duration (recurring orders)
- place similar order or list of orders without going through the entire ordering process (repeat orders)
Creating Subsets of Orders
The Standard list of orders of a care facility can be considered as a mother list of orders. It is made up of sub-categories belonging to various departments or units that is responsible for carrying them out i.e.:
- Clinical
- Laboratory
- Radiology/Imaging
- Endoscopy
- Pharmacy
- Dietary
- Supplies
Each of these main categories can be further classified into sub-sets based on criteria such as
- the sub-unit performing them,
- function or purpose from the requestor’s point of view
These are presented to users as drop-down or search lists derived from reference tables. Indeed, orders made by users can be reclassified on reaching the departments or units performing them as order lists for units, teams or machines. For example laboratory orders can be sub-classified into lists into:
- Anatomical pathology
- Histology
- Cytology
- Biochemistry
- Routine
- Specialized tests
- Immunology
- Hematology
- Routine
- Specialized analysis
- Blood banking
- Microbiology
- Bacteriology
- Virology
- Mycology
These sub-classifications are made based on how departments or unit within the facility organize their work.

Clinical users, on the other hand may want to create sub-sets of orders according to clinical purposes. The use of ‘order sets’ is discussed later and in the article on SOP/Care plans.
Order Details
When additional information needs to be provided with the order itself, this should be done by attaching the order details in the data-entry form defining additional specific information.
These details relates to:
- Instructions
- Information about the case
Instructions may relate to the following:
- Priority / Urgency (routine or stat)
- Timing
- Frequency (once or repeated at intervals)
- Responsibility of performing tasks
- Method (e.g. for drugs: route of administration)
- Other specific instructions
The order entry form should be designed to be customized to the type of order. For example orders for vital signs should allow the care provider to select the usual frequency from a list. For drugs, the recommended dose, frequency, interval and mode of administration should be given.
Information regarding the case should as far as possible be derived from data already collected elsewhere by the care provider (summaries created through a query of the database). This obviates the need for clinicians to write detailed information to go with the orders. Reminders regarding the patient’s physical condition and mental status or ability to communicate is helpful for some tasks.
Order Entry Mechanisms
There is a facility to allow or disallow care providers to place orders in ad hoc manner as and when necessary. When choosing an order, the user should be able to filter the orders by category and sub-categories so that the choice is made from the shortest list possible. The search for an order from the reference table can be made by typing in key letters. The user is able to create his/her favourite list of order sets and individual orders.
Each instance of an order made is given a unique system generated request number (accession number). The OERRS have the ability to print requisitions and specimen labels on placing the order and reprint these even while the orders are being processed.
Control of Use of Orders
Care providers can be allowed to or prevented from making certain orders based on the privileges accorded to them. Some orders may require verification. Hence, when an order is made by junior staff the application requests for a countersignature from a more senior staff before allowing the task to be carried out.
Orders must be made in the context of provision of care i.e. during a visit and in relation to a specific encounter. This rule ensures that the care provider demonstrates the indications for the order and is aware of the implications of making the order. Another important reason is that charges and the bill must be for tasks provided during the period when the service is provided.
Use of Order Sets in Patient Care Plans
The OERRS/CPOE has the facility for enabling users to place orders as pre-defined sets. These grouped orders called ‘care sets” or “order sets” constitute the main mechanism for the execution of Care Pathways and Care Plans (discussed in another article). A care-set is made up of a combination and permutation of orders/tasks. Care plans, hence care sets/order sets can be selected by the clinician from a list based on the diagnosis. the care provider is given the choice of activating or inactivating some or all of the orders or placing additional ad hoc orders. (Refer to section on Care Plans). Care plans, care sets or order sets can be selected by the clinician or automatically triggered based on rules.
Avoidance of Duplication
The application software is able to recognize a duplicate order and also provide an alert e.g. when more than one similar order is ordered within a defined time interval or based on any other criteria.
Use of Work Lists to Assign Responsibilities
The OERRS/CPOE also functions as the mechanism for task assignment. The tasks are assigned to the service unit/facility, resource or person responsible for performing them. These are presented as Task lists (Work lists/Queues) that can be assigned to:
- a service unit
- a category/group/team of care providers
- an individual care provider
- a machine
Duties and responsibilities can be assigned as defined by the care plan. (Tasks can also be routed by indicating who is to perform it in the order detail). Task-lists are then created for the relevant clinical, clinical support or administrative staff. The tasks are then completed in turn and results, in the form of various types of data (numerical, text or images), are sent for storage in the database and transmitted to the clinical units making the requests.
For samples (tissue or body fluid) sent for tests, each sample is labelled as belonging to a patient and a unique identifier is associated with the sample (automatically generated accession number which is usually a composite of date and serial number for the day). For this a bar-code labeling system is indispensable. The order entry part of the system allows clinicians to place orders that would be sent across to the receiving Clinical Support System.
The system has a facility to detect failure to perform the task at the time/date due and indicate the status as “overdue”.
There is a facility to cancel pending or overdue tasks, both manually when it is no longer required and automatically when the visit ends, with the exception of future orders.
There should be a facility to transfer tasks created in OERRS to clinical support service applications for e.g. Laboratory Information System, Radiology Information System and Pharmacy Information System through integration or interfacing.
Creation of Worklists

Automation of Work Processes
In some instances task and task lists can also be assigned to machines, devices or instruments so that processes are automatically started (after a manual initial set up) and regulated requiring no involvement of workers except for validation. Examples of such devices are monitoring devices, ventilators, IV infusion pumps, chemical analyzers, sterilizers, printers, copiers and scanners.
This automation should be achieved through machine-system interfaces using universally accepted interface/inter-operability standards combined with the use of bar codes, bar-coded labels and bar-code readers/scanners.
Providing Guidance & Warnings of Expected Complications
Decision support information and work instructions (order details) can be appended to the order. These include:
- Assigning urgency or priority
- Integration with scheduling
- Addition of Order details (Person ordering, Location of patient, indication)
- Attachment of instructions on Patient preparation
- Attachment of Patient education and instructions
- Provision of guidance, work instructions or reminders
- Provision of Warnings on Expected complications
RESULT REPORTING
The OERR application supports the sequence of processes of Order-Task-Result-Data entry thus ensuring that tasks are performed and results of the outcome are recorded. Tasks are only considered complete if the outcomes are recorded in any of the following manner:
- Recording of findings or results into a form or table (direct charting) and signing it off
- Direct transfer of results from machines to the database (machine-system interface)
- Acknowledging the completion of the task as “task done” (where no results need to be recorded).
- Acknowledging failure of performance or non completion of the task after being started, as “abandoned” or “not completed”
- Cancellation of the task
Where results are produced, a form or chart (containing one or more data fields) is made available to document them. The forms should contain data fields of various data types (text, numeric, images etc.). Results should be sent and stored in the database once validated or confirmed by the person performing the task. Results may also be transferred directly from machines to the database (machine-system interface).
Results should be displayed at an appropriate location in the CIS. The display should have capability of providing alerts regarding the results (normal/abnormal) and whether they have been read.
Persons assigned to perform the task are able to record the status of tasks as pending, in progress, performed, completed (successfully), incomplete, failed, re-scheduled or cancelled. The status is displayed accordingly to the care providers and other authorized users.
Order-Task Status as Quality Control of Process Performance
Orders are tasks yet to be performed. A the beginning the task status is considered to be ‘ordered’. Subsequently, the status indicates the various stages of the work flow ending with completion. The tasks may or may not be performed for various reasons or performed but failed to achieve its aims. At any time there is only one status. The terminology denoting the status is different for different types of tasks. Documenting or validating results are part of the task and the task is not considered done until the result is dispatched to the database.
Details for laboratory, imaging and pharmacy orders will be discussed further in the corresponding sections.

A view of the status of tasks will let care providers know which processes has not been completed delayed or not even ordered. The status acts as a control mechanism to ensure conformance to the Care plan. The expected interval between ordering of a task and its performance can be calculated and given the status delayed. A list of such tasks can be presented to the care provider team as a reminder.
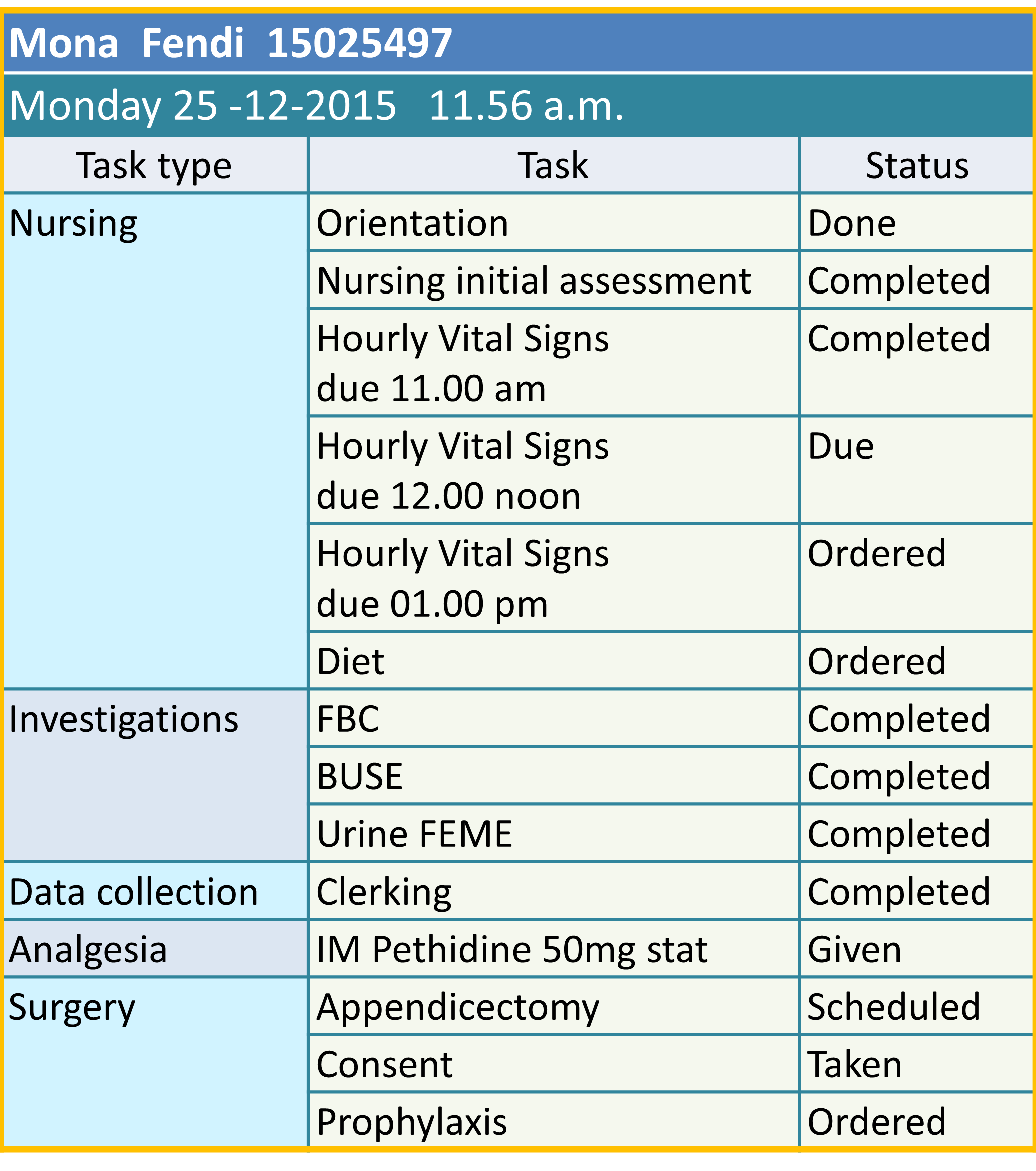
View of Status of All Tasks for a Patient at the Current Date and Time
View of Status of Orders and Tasks of Patients Undergoing Endoscopy on a Particular Day

Linking Completion of Tasks to Charges
The application passes information regarding the completion of a task to the Charging-Billing-Payment Application. Each order carries an order ID, a charge code and other data regarding charges. For the instances when charges are based on unit of work done, the charge value is assigned to the task using a charge code. Once the task is performed a message (containing the charge code) need to be sent to the charging-billing system to add the charge to the bill.

Link Between Order Entry and Charging-Billing Application
Linking Supply of Items with Inventory System
Where an order is a request for the provision of supplies, persons assigned to perform the task is able to record type and amount of items supplied. The recipient is able to acknowledge that the items have been received. These data should be capable of being tied to an Inventory system.

Hello Sir, I have a question related to the description you made and I would like some precisions about the functional scope of the PMS and CPOE (above). The CPOE description above is quite clear and in a previous page you indicate that CPOE is similar to a bridge managing the cooperation between CIS and CIS support subsystem.
In my understanding CIS is actually playing a role orchestra conductor for everithing related to car plan taking place within the hospital organisation. CPOE is the means to realize the necessary communication in between the different components, but it also requires specific functions like you have well described.
This brings me to my question which is related PMS, which includes as well “planning and resource allocation”, what are the differences you make between of functions of PMS and CPOE which seem similar to me? how should we see the things actualy?
Do you see planning/resource allocation of PMS as specialization of same functions of the CPOE which then makes this system as bridging system of the PMS and CIS.
Thank you in advance for your feedback.
Best regards
Cédric
LikeLike
Thanks for reading my articles and for your comment. I appreciate them.
The Patient management System is an administrative system sometimes also called PAS. It receives data from CIS and CPOE. It does not offer the functionality to initiate orders. The resource allocation in PMS relates to directing the patient to the right service unit or department based on the scheduling application. We can actually link orders to scheduling such that when an order is made it is also scheduled. For example a follow up visit or an admission is ordered, it can be scheduled. On arrival to a clinic, the care provider further assigns patients to rooms, care providers, machines etc. that has already been scheduled.
Further on, he/she is guided by multi-patient tasks lists (all attendees for the day) and task list of individual patients (if made earlier through future orders). Otherwise the assignment is made after the patient has been attended to. At this point the assignment is not part of the PMS. The task list originates from orders made by care providers, as care progresses, in the CIS through the CPOE. The CPOE is part of the CIS. Orders are relayed to relevant sub-applications and units including Billing-charging useful especially if a pre-pay approach is used i.e. no further care is provided without paying first.
I will edit my article based on your comments.
I am almost completing my article on care plans which though yet to be finished, you can view at https://drdollah.com/sops-and-care-plans/ .
LikeLike
Thank you so much for the precision and your article on Sops/Care plan that makes to me the functional scope (PMS and CPOE) and flows more clear, for me. That helps me to pursue my exercise of modelling this process and supporting application function and system with Achimate.
LikeLike